A TMD Case Study
The patient is a 78-year-old female who presented as a referral from her ENT due to TMJ pain.
This patient experienced significant tooth pain as a young adult, and multiple teeth were extracted. Due to numerous edentulous areas, the patient lost all posterior stops and began to function solely on her front teeth. The resulting occlusion led her to lose the vertical dimension of occlusion. I suspect that the asynchronous loss of teeth without replacement led to a chewing, clenching, and resting position that put unusual stress on her left jaw joint. This chronically over closed position and intermittent success with removable partial dentures led to her degenerative joint disorder. The patient has suffered on and off from myalgia of various muscles of mastication and arthralgia in the left joint.

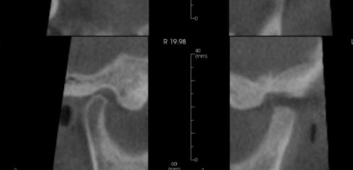
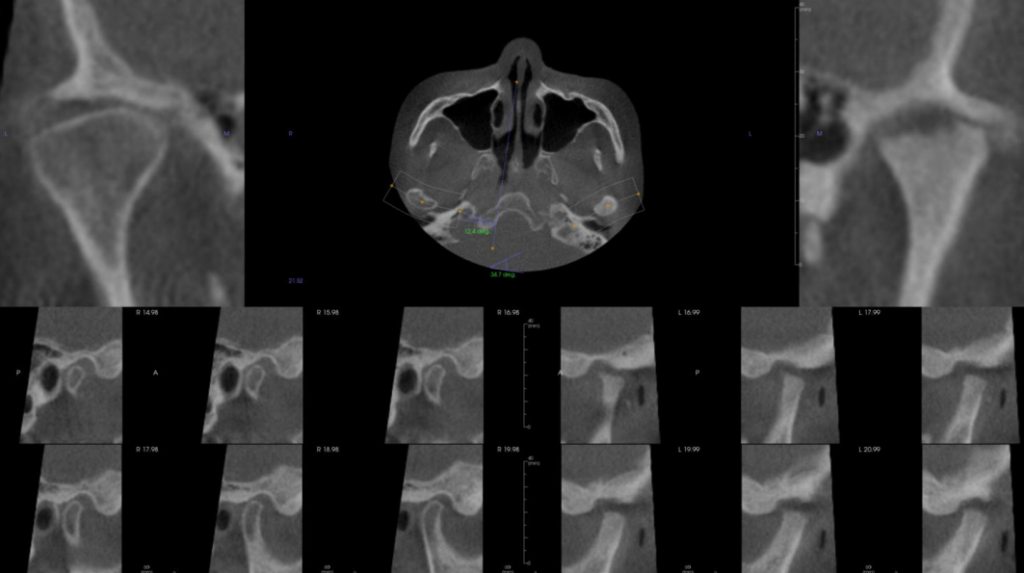
This lovely woman came to me for a solution to her pain. After obtaining diagnostic records, including CBCT scan, it was apparent to provide this patient with relief. We needed to open her up and test a different vertical dimension. To do this, I choose a two-splint technique. One splint is a daytime splint designed to bring the condyle down and forward, specifically more on the left joint than the right. The second splint is a nighttime sleeping appliance also intended to hold the jaw down and forward and to help quite the muscles of mastication in hopes that they would no longer pull as aggressively on the condyle.
After three months of 24-hour splint wear, the patient reported only mild discomfort 2 out of 10 compared to 8 out of 10 before treatment. The patient’s vertical range of motion improved from 36mm to 40mm, as well as an increase in her range of motion to the right side. At this time, we began the weaning process by limiting daytime wear. We also advised her to see her general dentist to restore her to a typical vertical dimension. I recommend doing this first through the aid of removable partial dentures. If, over time, she proves to be stable at this new vertical dimension of occlusion, consider replacing partial dentures with implant retained teeth. As a side note, most patients do not need any dentistry to achieve maximum medical improvement. Still, in this case, since she was missing so many teeth and had over closed on her remaining teeth, dentistry is definitely in order. The rationale for not immediately going to implant-retained teeth is one of risk. In my opinion, six months of testing a new vertical on a patient with such stark degenerative joint disease is too risky for the large investment of time and resources.
I hope this case helps you the next time you run into a similar situation.

If you are interested in referring a patient to Dr. Christina Cairns please visit my practice website with the following link, to download a referral sheet, electronically refer or just learn more about Colorado Springs Sleep Apnea & TMJ Solutions: Sleepishealthy.com